


Introduction
Eating disorders are illnesses of disconnection. They thrive on shame, guilt, secrecy, and silence—pushing strugglers away from the very people who could be their strongest support. Families, in turn, often feel powerless and retreat to protect themselves from conflict or pain.
In the past, treatment models even endorsed this separation. The infamous “parentectomy”—the removal of parents from the treatment process—was once considered necessary for healing. Today, we know better. Research consistently shows that family involvement improves recovery outcomes (Lock & Le Grange, 2019; Eisler, 2005). Families are not the enemy; in most cases, they are one of the most powerful protective factors against relapse.
And yet, in practice, strugglers are often encouraged to set boundaries that keep families at arm’s length, and families are told to “step back” to avoid enabling. While boundaries can be protective, when used as avoidance they reinforce the isolation in which eating disorders thrive.
In my experience as a family coach, I have rarely seen wounds close completely by running away from family. While there are extreme cases where separation is needed, most often recovery is stronger, more sustainable, and more hopeful when families learn to heal together.
Why Family Connection Matters
Eating disorders disconnect strugglers not just from food and body, but also from people. Shame and guilt convince them they are a burden. Conflict convinces families they are helpless. Recovery requires reversing that pattern—replacing isolation with connection.
- Shame dissolves in connection. A struggler who believes they are “too broken” can begin to feel worthy again when a parent says, “I’m here with you, no matter what.”
- Accountability fosters progress. Sitting alone with the eating disorder feels impossible. Sitting with a parent who says, “I’ll stay here until you’re finished,” makes the unbearable manageable.
- Trust repairs resilience. Eating disorders often fracture family bonds. But when apologies are exchanged and trust is rebuilt, the family itself becomes a source of strength.
Why Strugglers Sometimes Resist Family Involvement
One of the most common reasons my clients tell me they resist involving family is fear of being hurt.
Many strugglers say:
- “I’ve tried to let them in, but the same fights always happen.”
- “I want their help, but it just makes me feel worse.”
- “They don’t understand me, and it feels easier to do this alone.”
These are not excuses; they are honest experiences. Old patterns can resurface quickly: criticism, overprotection, nagging, or withdrawal. Strugglers may feel trapped between needing connection and fearing more pain.
It’s also important to recognize that sometimes the family has not actually done anything “wrong.” Instead, the struggler is facing their own demons. Shame, guilt, and embarrassment convince them they are unworthy of such a good family. They may feel they are a disappointment, that they can’t live up to expectations, or that they are—without better words—“a loser.” Some strugglers describe feeling as if their very presence shames their family.
In families with siblings, a struggler may feel stuck in a long-standing competitive relationship, always believing they were “less than” or never good enough. This could happen among friendships as well. In these situations, therapeutic family work is about reframing the internal dialogue of the struggler—helping them see that worth is not conditional, and that love is not earned through achievement or comparison.
Family work also requires validating the strugglers’ feelings, not dismissing them. But validation does not mean replacing emotional connection with material gifts. Too often, parents who find it difficult to confront their own emotions, default to buying things—clothes, trips, or other materialistic items—believing it demonstrates care and compassion. For the struggler, this can reinforce the belief: “I am only worthy when something is bought for me.” ” They only know how to love me with money.” It conditions connection to be transactional. This doesn’t mean never buy or treat the struggler with material items. It means not as a way to buy connection.
True connection must come from shared presence—the ability to sit together, talk, or simply enjoy each other’s company without materialism camouflaging the relationship. Recovery deepens when families learn that their greatest gift is not what they buy, but how safe, respected, and valued they help their loved one feel in everyday moments.
Another key factor is the way communication is delivered. I often remind families: “It’s not what you say, it’s how you say it.” We are living in a generation that communicates differently than many years ago. Today’s young adults—and even many adults in therapy—are attuned not only to words but also to tone, pacing, and sensitivity. Speaking in ways that are too blunt, too clinical, or too hard-edged may feel almost unbearable in today’s relational culture.
When a parent says, “You have to eat or you’ll die,” it may be factually accurate but land as harsh and shaming. If instead the parent says, “I know eating feels impossible right now, but your body truly needs this food to survive—and I will sit with you through it,” the same truth is spoken, but with validation and empathy. That shift in tone fosters dialogue rather than shutting it down.
Simply changing one’s delivery—balancing realism with compassion—can make the difference between a struggler leaning in or retreating into silence. Communication that combines honesty with validation provides an avenue for discussion instead of sending someone into defensive shutdown mode.
Have you shared any personal stories? When parents never share personal stories about their own upbringing, children often experience them as distant or “unreal,” as if they have no background story of their own. This absence of vulnerability can create a wall between generations, leaving the struggler feeling isolated and misunderstood. In recovery, hearing about a parent’s challenges, fears, or even mistakes humanizes the parent and opens a doorway for dialogue. These conversations give the struggler permission to share their own story more openly—reminding them that imperfection is part of being human and that connection grows through shared experience, not silence.
Strugglers are usually depressed and angry. Adolescents in particular often use oppositional and defiant behavior as a form of communication during the recovery process. When words feel too vulnerable or shame-filled, resistance becomes their language. At times, defiance is less about rejecting treatment and more about expressing anger, resentment, or helplessness toward parents. It can function almost like a punishment: “You hurt me, so I will hurt you by refusing to cooperate.” This oppositional stance is often intentional, a way of manipulating dynamics to regain a sense of control or to make parents feel the same frustration the adolescent feels inside. Recognizing this behavior not simply as “bad attitude” but as a maladaptive expression of pain allows therapists and parents to redirect the energy—validating the underlying anger while also setting firm boundaries that protect both the struggler and the family relationship.
The Cave Analogy
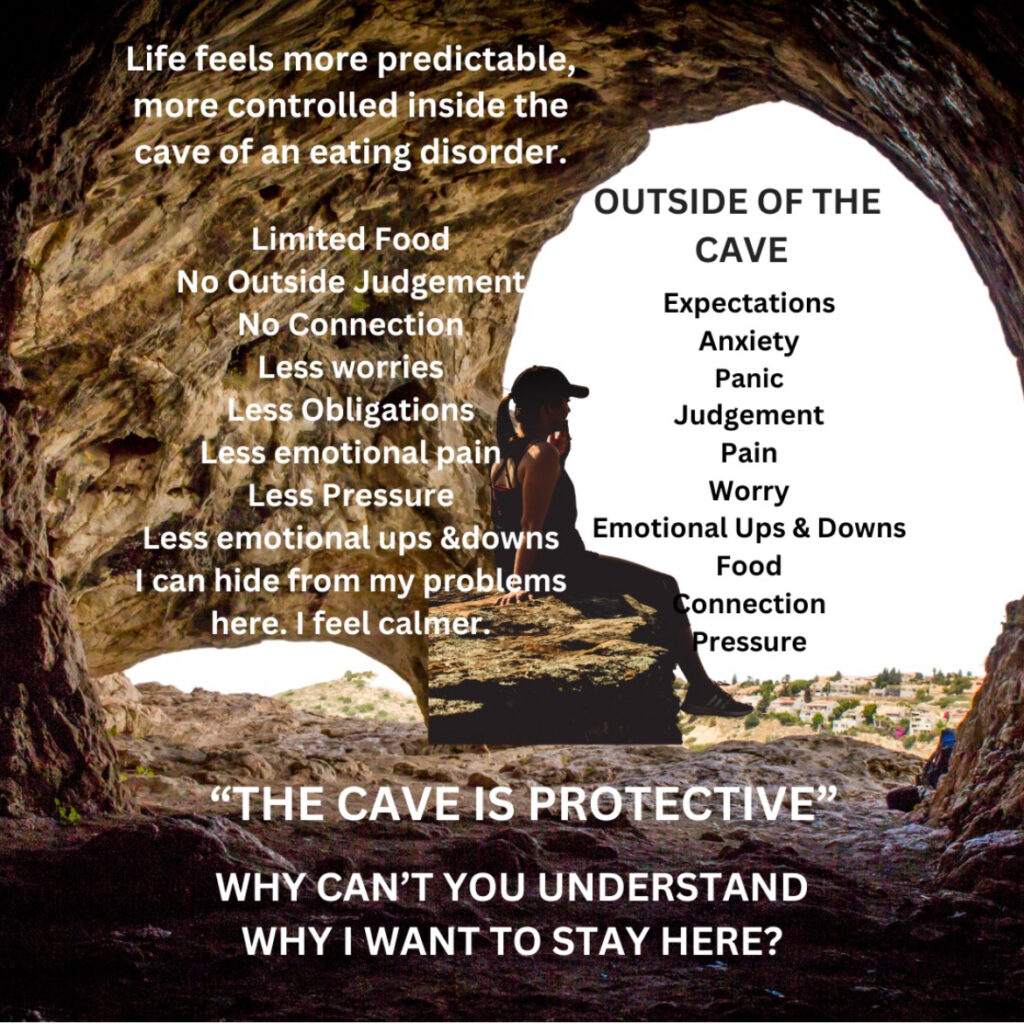
I often use an analogy with clients: imagine the struggler hiding in a cave. Inside the cave it is quiet—no outside noise, no conflict, no painful conversations. But there is also no food, no connection, no joy, no quality of life. Sometimes, the cave even offers numbing comforts—alcohol, drugs, or the eating disorder itself—to dull the pain.
Another reason some strugglers stay in the cave is that they are noticed there. In a maladaptive way, the illness itself draws attention. Families visit the cave, worry about them, and spend more time around them. Outside of the cave, when recovery begins, life often “goes back to normal”—school, work, other siblings, other responsibilities. Without an intentional effort to maintain healthy connection, the struggler may feel invisible again. And we all know the painful truth: at times, bad attention feels better than no attention.
I have seen many families who, during the height of illness, make extraordinary efforts to buy time and spend more moments with their loved one. But as recovery progresses, those moments disappear. The struggler may then conclude that the only way to keep love, time, and attention is by slipping back into maladaptive behaviors.
Of course, this is not always the family’s fault. Some strugglers have what feels like an endless tank—an insatiable need for validation that no one else can fill. In these cases, it is the responsibility of mental health professionals to help the struggler explore deeper issues of self-fulfillment, self-worth, and life satisfaction—teaching them that connection cannot always be sustained through external validation.
Sometimes expectations of family become excessive, fueled by anger or resentment. In those moments, strugglers may unconsciously punish their family members, blaming them for their emptiness or low self-esteem. Here, too, the therapist’s or coaches role is essential: helping the struggler distinguish between healthy connection and unrealistic demands, while supporting families in setting compassionate but firm boundaries that protect everyone’s well-being.
This is the heart of recovery work. The family’s job—by doing their own work—is to create a safer, more balanced environment outside the cave so the struggler dares to step out. The therapist’s and life coach’s job is to help the struggler identify what prevents them from leaving the cave and, just as importantly, what keeps pulling them back inside. That is the main work of recovery: learning to step out of hiding and stay engaged, even when it’s hard.
When Families Resist Change
It’s not only the struggler who avoids. Many families also resist the hard relational work recovery requires. Parents may say, “We’ll support her once she eats, but we won’t do therapy.” “Why did this become our problem? We have done everything to help her?” Siblings may withdraw, exhausted by years of tension. Spouses may feel hopeless and choose self-preservation.
Another layer of resistance comes from how families perceive communication today. Many parents or relatives see the emphasis on sensitivity, tone, and validation as “psychobabble” and resist what feels like soft or unnecessary discussion. They may say, “We didn’t need this nonsense in our day.” But family coaches and therapists must gently but firmly remind them: Times change and recovery is more important than our egos or our resistance. Speaking with compassion is not weakness—it is a therapeutic tool that makes dialogue possible.
At the same time, strugglers must also be held accountable. Softer, more compassionate language should not be used to manipulate conversations or avoid responsibility. I often tell both my clients and my families: “Never mistake my kindness for weakness.” Compassion does not mean unlimited tolerance. We all have thresholds. This truth, spoken kindly, becomes a boundary in itself—a reminder that recovery requires honesty, accountability, and respect on both sides.
Both the struggler and the family must be willing to grow: families by softening their approach, strugglers by not abusing it. This balance fosters a new playing field where real communication and healing can take place.
When Boundaries Help—and When They Hurt
The question I often ask my clients is: “Is this boundary protecting you—or protecting the eating disorder?”
That distinction matters. Boundaries are vital when they protect dignity, create safety, or support autonomy. But too often, what gets labeled as a “boundary” is actually avoidance—a way of protecting the disorder.
Many families and therapists focus heavily on meal-related boundaries—whether a parent can sit at the table, whether food talk is allowed, whether accountability at meals is acceptable. But meals are not where the true focus needs to be. Recovery is not just about food; it’s about life.
The boundaries that matter most are those connected to real-life functioning and self-worth:
- Critical language that reinforces shame.
- Expectations higher than what the struggler can achieve right now.
- Fear of failure that prevents trying.
- Not feeling good enough, which fuels the eating disorder’s grip in the first place.
These are the areas where boundaries provide true protection—helping the struggler feel safe enough to step into life while not reinforcing the disorder.
The challenge is that eating disorders speak through the ED lens—food, calories, weight, and body—because expressing vulnerability through the language of real life (failure, shame, not enough) feels too raw. A demand like “I don’t want my parents at meals” may really mean “I feel like a failure when people are watching me.” Without exploring beneath the surface, therapists may validate avoidance without realizing they are reinforcing the disorder.
Boundaries, then, should not be about avoiding meals, but about creating space for the struggler to express—and for the family to respond to—the deeper fears that drive the illness.
The ARISE® Model: Healing Together
The ARISE® Family Intervention Model embodies this approach. It invites families into the recovery process from the very start, viewing them as the healing system rather than the problem.
Core Strengths:
- Inclusion from the Start – The struggler is invited transparently from the first step, reducing shame.
- Collaboration Over Confrontation – Families learn new communication patterns to avoid falling into old traps.
- Sustained Involvement – Families remain engaged throughout treatment and aftercare, lowering relapse risk.
- Boundaries as Bridges – Limits are reframed as structures that keep people safely connected rather than apart.
Research shows ARISE improves treatment engagement and sustains family involvement more effectively than traditional models (Landau et al., 2000; Garrett et al., 2018).
Families as Protective Factors
Studies confirm what I see daily: when families stay connected, recovery outcomes improve.
- Family involvement reduces relapse (Couturier et al., 2013).
- Relational repair increases resilience (Hibbs et al., 2015).
- Social support predicts recovery across ages and diagnoses (Tiller et al., 1997).
Beyond research, I’ve witnessed families who once fought at every meal learn to sit together in peace. I’ve seen strugglers who feared family involvement realize that, with new skills, their parents could be allies instead of enemies. And I’ve seen families who initially resisted therapy discover that doing their own work transformed not only the struggler’s recovery, but the health of the entire family system.
Conclusion
The insights shared in this article may resonate deeply with some families—and feel less applicable to others—and that’s entirely valid. No two recovery journeys are the same, nor should they be. As you move forward, it’s crucial to filter and apply what truly supports your family’s healing, discerning between what encourages growth and what doesn’t.
Many individuals receive multiple psychiatric diagnoses during the course of their eating disorder—often more than a dozen—reflecting how severe distress can create overlapping symptoms. However, research suggests that with nutritional rehabilitation and family recovery, a substantial portion of these comorbid diagnoses may resolve or diminish. For instance, psychiatric comorbidity occurs in as many as 55% of adolescents and up to 96% of adults with eating disorders, but not all of these conditions remain post-recovery bmcpsychiatry.biomedcentral.com+4frontiersin.org+4jeatdisord.biomedcentral.com+4.
This doesn’t minimize the reality of persistent mental health challenges for some—it emphasizes the importance of ongoing, sensitive evaluation. When we assume a diagnosis is permanent, we risk over-pathologizing behaviors that may be secondary to the eating disorder itself. Conversely, we must also be vigilant in identifying co-occurring conditions that genuinely require independent treatment.
Ultimately, recovery flourishes in connection, not isolation. It requires staying connected through compassion, boundaries, honesty, and flexibility. Families may not always get it right—but persistence, humility, and presence matter most. Healing doesn’t happen in solitude—it happens in relatability. Wherever your family is in this journey, may you find the tools and courage to create enduring connection together.
References
- Couturier, J., Kimber, M., & Szatmari, P. (2013). Efficacy of family-based treatment for adolescents with eating disorders: A systematic review and meta-analysis. International Journal of Eating Disorders, 46(1), 3–11.
- Dimitropoulos, G., et al. (2015). Experiences of parents of adolescents with eating disorders: A qualitative study. International Journal of Eating Disorders, 48(6), 791–800.
- Eisler, I. (2005). The empirical and theoretical base of family therapy and multiple family day therapy for adolescent anorexia nervosa. Journal of Family Therapy, 27(2), 104–131.
- Garrett, C., Landau, J., Shea, R. R., Stanton, M. D., Baciewicz, G., & Brinkman-Sull, D. (2018). The ARISE® comprehensive care with invitational intervention: Engaging reluctant substance abusers in treatment. Journal of Marital and Family Therapy, 24(2), 165–177.
- Hibbs, R., et al. (2015). Relational aspects of recovery from adolescent anorexia nervosa: Family members’ perspectives. European Eating Disorders Review, 23(4), 294–303.
- Landau, J., et al. (2000). Outcomes with the ARISE approach to engaging resistant individuals in treatment. Addiction, 95(10), 1365–1379.
- Lask, B. (2016). Why family involvement is essential in the treatment of eating disorders. Journal of Eating Disorders, 4(1), 14.
- Lock, J., & Le Grange, D. (2013). Treatment Manual for Anorexia Nervosa: A Family-Based Approach. 2nd ed. Guilford Press.
- Lock, J., & Le Grange, D. (2019). Family-based treatment: Where are we and where should we be going to improve recovery in child and adolescent anorexia nervosa. International Journal of Eating Disorders, 52(4), 481–487.
- Schmidt, U., & Treasure, J. (2006). Anorexia nervosa: Valued and visible. A cognitive-interpersonal maintenance model. British Journal of Clinical Psychology, 45(3), 343–366.
- Tiller, J. M., et al. (1997). Social support in patients with anorexia nervosa and bulimia nervosa. International Journal of Eating Disorders, 21(1), 31–38.
- Treasure, J., et al. (2007). Anorexia nervosa: A survival analysis. Psychological Medicine, 37(7), 1073–1080.
- Zaitsoff, S. L., & Taylor, A. (2009). Factors related to motivation for change in adolescents with eating disorders. European Eating Disorders Review, 17(3), 227–233.*
