

By Iris Epstein, RDN, CEDS, ARISE Interventionist
One of the hardest things for families to understand about anorexia nervosa is why it persists. Why doesn’t the person just eat? Why, when they can clearly see the worry on everyone’s faces, do they continue down a path that is visibly destroying them? Why does someone who is articulate, intelligent, and accomplished in every other area of life seem completely unable to see what everyone around them sees?
The answer is not stubbornness. It is not vanity. It is not a choice. What sustains anorexia is a series of interlocking biological forces that together create one of the most self-reinforcing — and most misunderstood — disease states in medicine. And it begins with something most people would never expect: the brain’s reward system.
When Starving Feels Like a Reward
In the early stages of anorexia, restricting food and exercising excessively don’t feel wrong to the person experiencing them. They feel good. The brain registers these behaviors as rewarding — producing a sense of control, accomplishment, even relief. This is not a metaphor. This is the brain’s dopamine system, the same system involved in any pleasurable experience, responding to restriction as though it were something worth repeating.
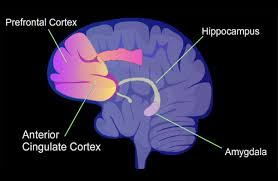
Over time, something darker happens. Those same behaviors stop feeling good and start feeling compulsive and even painful — yet the person continues doing them anyway. This is where a critical brain region called the anterior cingulate cortex, or ACC, becomes central to the story. The ACC normally acts as a kind of referee between reward and punishment — helping the brain recognize when something that once felt good has turned harmful. In anorexia, this region becomes underactive. The referee goes quiet. And without that regulation, the brain loses its ability to course-correct. The behaviors lock in. The disorder sustains itself.
Brain scans confirm this. People with anorexia show measurably reduced activity in the reward and decision-making centers of the brain compared to people without the disorder. And here is the hopeful part: as people begin to restore weight through nutritional rehabilitation, those same brain regions start waking back up. Behavior begins to normalize alongside brain recovery. This is powerful evidence that the brain can heal — but it needs fuel to do it, and it needs time. More time than most people, and most treatment programs, are willing to acknowledge.
Stress: The Hidden Engine
What most people don’t realize is that stress is not just a symptom of anorexia. It is one of its primary drivers and sustaining forces. When the body is in a state of chronic self-generated starvation, it produces persistently elevated levels of cortisol — the body’s primary stress hormone. And cortisol at sustained high levels is directly toxic to the brain. It damages the regions responsible for memory, flexible thinking, emotional regulation, and self-perception.
This creates a devastating cycle. The restriction produces cortisol. The cortisol damages the brain regions needed to recognize that restriction is harmful. The damaged brain continues restricting. The cycle deepens.
This is not the stress response of someone having a hard week at work. This is a chronic, physiological state of perceived emergency — the body convinced at a hormonal level that famine is happening, that survival is threatened, that every available resource must be conserved and controlled. The brain operating under that level of sustained stress is not the same brain that existed before the illness began.
How Long Does the Brain Take to Heal?

This is one of the most important — and most under-discussed — questions in eating disorder treatment. When a person begins nutritional rehabilitation, the brain does not simply switch back on. Recovery happens in stages, across different systems, over a timeline that is far longer than most people anticipate. Understanding this timeline is not discouraging — it is essential. It explains why stepping someone down from treatment too quickly is dangerous, and why a person who has reached a target weight is not yet a person whose brain has caught up.
The first two to four weeks bring some of the most acute and immediate changes. As consistent nutrition is restored, the most dangerous hormonal instabilities begin to stabilize. Cortisol starts to come down from its crisis-level elevation. Ghrelin — a hormone that becomes severely dysregulated during starvation and contributes directly to anxiety, hyperactivity, and obsessive thinking — begins to normalize. Basic electrolyte balance improves. These early shifts matter enormously because they begin to reduce the physiological state of emergency the body has been living in. The person may begin to feel slightly calmer, slightly less rigid. This is the brain’s crisis response beginning to downregulate. It is the very beginning of a very long road.
Between three and six months of consistent, adequate nutrition and sustained weight restoration, the hunger and satiety hormonal axis begins to meaningfully recover. The most critical hormone in this window is leptin — the hormone responsible for communicating fullness, metabolic rate, and reproductive function to the brain. In anorexia, leptin becomes profoundly suppressed. Until it is restored to functional levels, the brain continues to receive famine signals regardless of what the scale says. A person can be at a restored weight and still have a brain that believes it is starving, because the leptin signal has not yet caught up. This is a critical and frequently missed clinical reality. It is also why so many people relapse in early weight restoration — they feel recovered on the outside while their brain is still operating in survival mode on the inside.
Between six and twelve months, measurable structural brain recovery begins to occur. The gray matter loss and cortical thinning that malnutrition produces — the physical thinning of the brain’s outer layer that reduces its capacity for self-awareness, emotional regulation, insight, and flexible thinking — begins to reverse as nourishment is sustained. Brain imaging studies show measurable increases in cortical volume and thickness beginning around the six-month mark in patients who maintain weight restoration. However, full or near-full structural recovery — particularly in the prefrontal regions most responsible for insight, decision-making, and self-regulation — can take twelve months or longer, and in cases of long-duration illness may never be fully complete.
Beyond twelve months, the deeper neurochemical rewiring continues. The dopamine and serotonin systems that were reorganized around restriction do not simply reset with weight restoration. They require sustained nourishment, reduced stress, therapeutic support, and time to gradually reestablish healthier patterns of signaling. This is why therapy tends to become more effective — not less necessary — in the later stages of recovery. The brain is finally gaining enough structural and neurochemical stability to actually engage with and integrate therapeutic work. Trying to do deep psychological work in the early months of recovery, before this neurological foundation is in place, is like trying to renovate a house before the foundation has been poured.
Why This Is Different From Other Malnourished States
This is a question worth asking directly, because it gets to the heart of what makes anorexia neurologically unique. People undergoing significant weight loss through bariatric surgery or GLP-1 medications, or people losing weight due to cancer or chronic illness, can be just as calorically depleted as someone with anorexia. So why don’t they typically experience the same loss of perception, insight, and emotional regulation?
The answer is that in anorexia, malnutrition is not the only force at work. It is malnutrition plus something no other malnourished state produces in the same way — a perfect storm of converging forces that together create a uniquely devastating neurological picture.
People losing weight through medication or surgery are not experiencing restriction as rewarding. Their brain’s reward system has not been reorganized around not eating. They are not engaged in a daily, active suppression of their body’s hunger signals — a process that, over time, structurally damages the brain regions responsible for reading the body’s internal communication. They are not experiencing a meal as an existential threat that triggers the same brain response as physical danger. And critically, they are not fusing their identity with their illness — the point at which recovery feels not like getting well, but like losing who you are.
In anorexia, all of these forces converge simultaneously. Malnutrition. Chronic cortisol elevation. A reward system reorganized around restriction. The progressive silencing of the body’s internal signals. Identity fused with the illness. Each force amplifies the others. Together they produce brain changes that no other malnourished state replicates in the same way or to the same degree. A cancer patient is not treating their next meal as a survival threat. A bariatric patient is not experiencing hunger suppression as a core expression of their identity and worth. Only in anorexia does the brain become both the organ that is damaged and the organ that is actively, neurologically committed to continuing the behavior that damages it.
Nobody Asked for This
Perhaps the most important thing to understand about anorexia is how it begins. Almost never does it start with a desire to be sick. It typically begins with stress — a loss, a transition, a season of feeling out of control. Or it begins with innocent dieting, a simple wish to lose a little weight, the kind of thing millions of people do every year without consequence. Then, in a brain with a particular neurological architecture — one wired toward anxiety, perfectionism, and sensitivity — something shifts. The restriction starts to feel rewarding. The brain begins to reorganize. The disease takes over.
By the time the people who love them are alarmed, the person with anorexia is often already living inside a brain that cannot accurately perceive its own condition. They are not refusing help out of stubbornness. They are refusing help from inside a neurological state that has made the illness feel like safety, identity, and survival all at once.
Understanding this doesn’t make treatment easier. But it makes compassion unavoidable. And compassion — paired with early, sustained nutritional rehabilitation and appropriate therapeutic support timed to where the brain actually is in its recovery — is where healing becomes possible.
Nutritional rehabilitation is not one component of anorexia recovery. It is the biological prerequisite for all other recovery — the foundation upon which a healing brain can slowly, and with the right support, begin to find its way back.
If you or a loved one needs support for an eating disorder, reach out to the Nutrition Improvement Center (NIC) Today at 845-362-1300. Email us at ad***@***rd.com. Join NIC Academy Now by clicking on this link for a free preview of our course “The Dietitian Made the Menu…Now What?:
https://iris-s-site-e8dc.thinkific.com/products/courses/thedietitianmadehtemenufreewelcome
